TRAIN HARD.
STAYFOCUSED.
EARN TRUST.
Our obedience training uses a personalized
program tailored to your dog, combining a
balanced training approach with proven
techniques to support long-term success and reliable behavior.

Starting April 11, 2026, all students enrolling in Ghost K9 Academy Group Classes must attend Basic Training Orientation prior to their first group class.
Orientation Date | Saturday, July 11, 2026
Start Time | 9:30 AM
Location | Ghost K9 Academy, Stoughton, MA
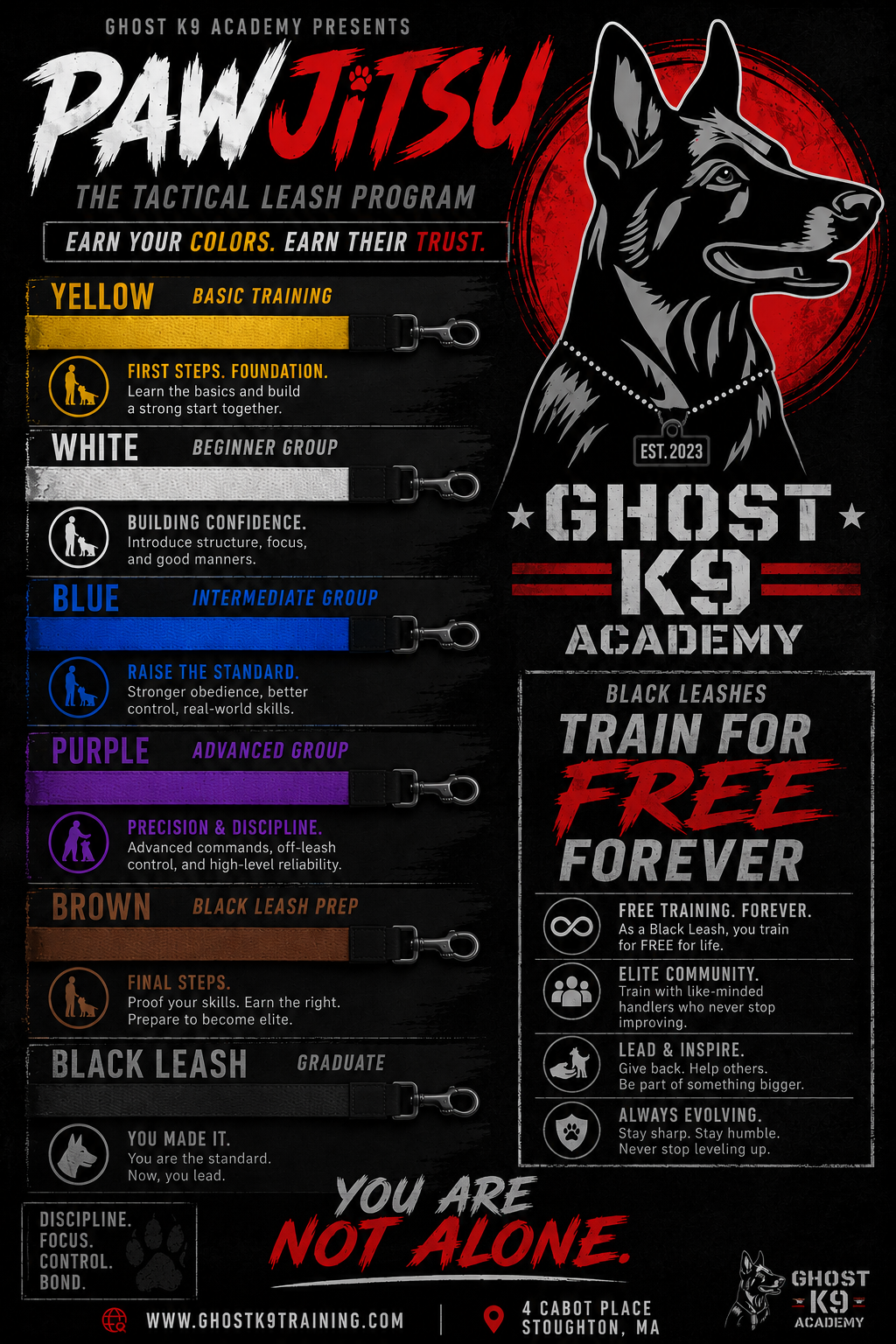
This class is attended without your dog and serves as a one-day orientation designed to set you up for success. During the session, we will review class rules and expectations, walk you through how to use the Student Portal, explain how scheduling works, and go over the required equipment. We’ll also introduce the Color Leash System and outline what you can expect as you progress through your training journey.
IMPORTANT
Depending on when you enroll, the time leading up to the Basic Training Orientation will be spent working one-on-one with an instructor to complete the prerequisite lessons required before attending this class. Once the orientation is completed, you will receive your official class schedule and be placed into the appropriate group training class. This orientation is held on the first Saturday of every month, and attendance is required prior to joining any group classes.

Coby’s Story
Stephen and his team are phenomenal. I enrolled my 120 lb Cane Corso in private and obedience classes and I couldn’t be happier with the results. As a large and strong breed, my Corso needed firm, consistent training—and that’s exactly what we got. The trainers were knowledgeable, patient, and clearly experienced with working breeds. From basic obedience to leash control and socialization, each class was structured and hands-on. What I appreciated most was the focus on positive reinforcement and building a strong bond between me and my dog. The trainers took time to understand my Corso’s temperament and tailored strategies that worked for him. Now, walks are calm, commands are followed, and guests can actually come over without being greeted by 120 pounds of excitement! Thank you Ghost K9.

Ollie’s Story
The draw for me to be apart of Ghost K9 Academy was the community. I wanted to be able to hike with my dog and go for a walk without my shoulder becoming dislocated. I cannot say it was easy but boy was it worth it. My 100lb lab mix Ollie is a different dog and now 7 months in we are at the fun stage. Steven and the entire staff are knowledgeable and invested not only in the dog but in me as the handler. I learned we are a team and Ollie feeds off me. There is still so much to learn and Ollie and I are excited to keep raising the bar. This program is well structured and builds each week. I get so many compliments on how well tempered and trained Ollie is. If you are willing to put the time and effort in, this place will show you the way.
